
Documenting Wounds
I was honored to present a webinar this past week for the Massachusetts Alliance for Care at Home. Wounds are always tricky, and its great to remind even your seasoned staff about the rules. One of the issues that we see day to day when we are reviewing charts is the lack of consistency in documentation from referral, through to the diagnosis coding, OASIS items, plan of care and wound care orders.
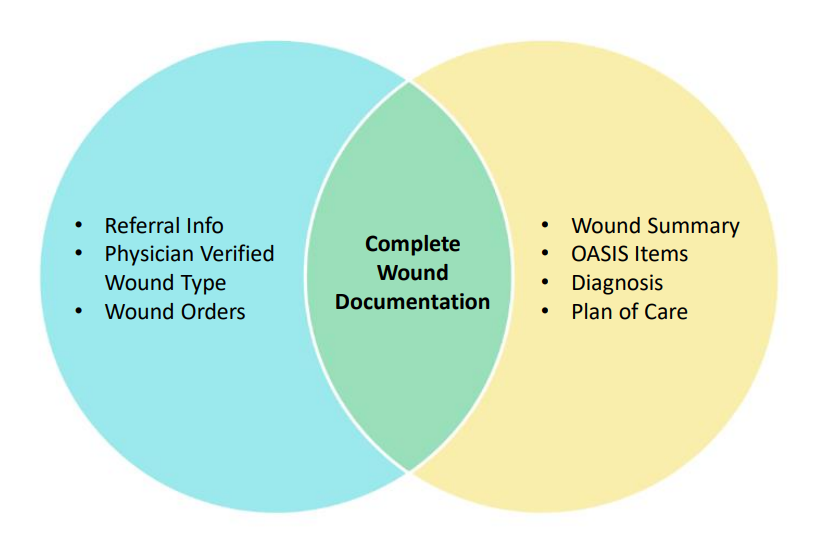
A complete order for wound care includes the following items:
Etiology of Wound
Wound location
Type of wound
Type of cleaning/irrigation solution
Whether skin prep is being used
Type of primary dressing being applied (hydrogel, hydrofiber, calcium alginate, etc.)
Type of secondary dressing being applied, if needed (ABD, border gauze, foam, etc.)
How dressing is being secured (tape, bordered gauze, etc.)
Wound care frequency
Clinicians Can Provide:
Laterality of Wound
Pressure Ulcer Wound Stage
As the highest paid clinical group, its important to get wounds documented correctly! You want to make sure your coders are coding wounds as primary, if appropriate, or secondary to capture the co-morbidity adjustment. 45 of the 98 (46%) comorbidity combinations that result in a high comorbidity adjustment are related to Skin. You need to make sure the eitology of the wound is verified by the physician, and that its the focus of care for it to be captured as primary. If its not the focus of care but its still being cared for or monitored for signs/symptoms of infection, capture it as a second diagnosis. You also want to make sure that your clinicians are documenting the wound in the OASIS items as the same etiology as the physician verified.
If you think your staff need a refresher on wounds, reach out to us. We would be happy to provide your team the education they need.
April 1st OASIS Changes
Effective April 1, 2026, OASIS is being updated from Version E1 to Version E2. Here is summary of what’s changing between OASIS-E1 and OASIS-E2 that takes effect April 1, 2026:
Item Replacements / Modifications
A0810 (Sex) replaces the previous M0069 (Gender) item — refining demographic data in line with updated CMS terminology.
A1255 (Transportation) replaces A1250 (Transportation) — revised to align this item with similar transportation elements used in other CMS assessment tools.
Several editing and skip-logic changes occur — for example, skip patterns related to physician-ordered start or resumption of care tie into the new Transportation item logic.
New Items Added
CMS is adding a few items to the Resumption of Care (ROC) time point to enhance risk adjustment and multidimensional assessment:
B0200 (Hearing) — hearing ability.
B1000 (Vision) — vision ability.
A1110 (Language) — preferred language and interpreter needs.
Removed Items
O0350 (Patient’s COVID-19 vaccination is up to date) is removed from the dataset.
The original A1250 Transportation item is retired with the addition of A1255.
In short, OASIS-E2 keeps much of the structure from E1 but updates and standardizes key items (like sex and transportation), adds new data elements at ROC, removes outdated items (like COVID vaccination), and adjusts skip logic and edits to better align with CMS quality reporting and interoperability goals.

OASIS Fall Reporting (J1800 & J1900)
What Counts as a Fall?
Unintentional change in position to ground or lower surface
Includes intercepted falls
Includes falls due to overwhelming external force
Does NOT include anticipated loss of balance during supervised balance training
Injury Definitions
Injury (Except Major):
Includes but is not limited to skin tears, abrasions, lacerations, superficial bruises, hematomas, and sprain; or any fall-related injury that causes the patient to complain of pain.
Major Injury:
Includes but is not limited to traumatic bone fractures, joint dislocations/subluxations, internal organ injuries, amputations, spinal cord injuries closed head injuries, and crush injuries
Important Update:
Pathologic fractures (confirmed by physician) are NOT major injuries for J1900C.
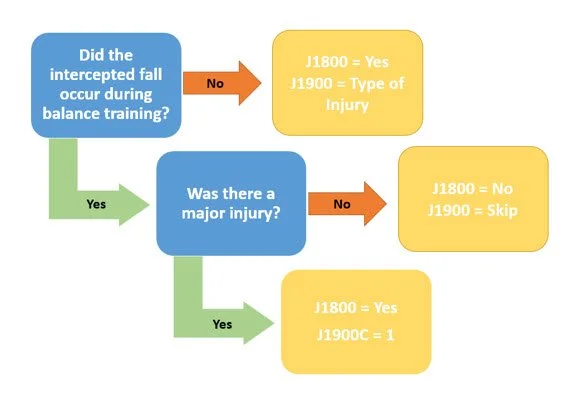
Special Scenarios
Intercepted Fall vs Falls in Balance Training
Patient stumbles during ambulation and therapist prevents fall → IS a fall
J1800 = Yes
J1900 = Answer per injury type
It was an anticipated loss of balance during therapeutic balance training→ NOT a fall
If a major injury results from a fall or intercepted fall that occurs when a clinician is intentionally challenging a patient’s balance during balance training, it would be reported as both a fall and a major injury in J1800 and J1900.
Outsourced Coding & OASIS Services: Key Questions to Ask Your Coding Services Partner
Not all outsourced services companies are created equal. You want to ask questions related to your future partner’s staff qualifications and experience, both in the industry and in your specific system(s).
• How long have you been providing OASIS review and coding services?
• What is the background and certification(s) of your coders/reviewers?
– Coding Certifications ( HCS-D, BCHH-C)
– OASIS Certifications (HCS-O, COS-C, COQ-S)
• Do your reviewers have clinical experience in home health?
• Are your staff familiar with PDGM, VBP, and OASIS-E requirements?
You want to make sure that your outsourced services provider is following the most current coding and OASIS changes, is aware of the Medicare COPs, and that they are regularly auditing their own work (so you don’t have to!)
• How do you ensure coding and OASIS reviews are compliant with coding guidelines and CMS regulations?
• How do you stay updated with changes in regulations and guidelines such as OASIS updates and Coding updates?
• Is there a quality assurance process? Who performs the QA and how often are coders audited?
Coding and OASIS are not only a crucial part of your revenue cycle, but they are also tied to your timely submission of OASIS and claims. Don’t let your Outsourced Services Provider add unnecessary days to the process, but also make sure you understand their process enough that they are not just “pushing charts” through for timeliness vs. accuracy.
• What is your average turnaround time for OASIS and coding reviews?
• Do you offer expedited reviews when necessary?
• Are your services available on weekends or holidays?
• What is your process and turnaround time for charts that go on hold?
Outsourcing your Coding and OASIS review doesn’t mean you don’t need to actively participate in the process. You, as the agency, should have a dedicated staff member(s) to oversee the communication process and ensure that your outsource service provider is meeting your expectations.
On the other hand, you should also have a point person you can contact.
• How do you communicate with our staff when questions or clarifications are needed?
• What is the expectation of turnaround time once that information has been provided back to the coder/reviewer?
• Do you assign dedicated reviewers to maintain consistency and develop a relationship with the agency staff?
• Will we have a point of contact or account manager?
• Do you, as the agency, have a point of contact available to your outsourced services provider?
As part of the implementation process, you should map out a clear procedure that both sides are going to follow, and know who is responsible for which part of the process. This will reduce or eliminate any confusion as you get started with your new partner.
• How do you access our documentation (e.g., EMR integration, secure upload)?
• How do you determine which charts are ready for review?
• Are you familiar with our EMR system? (e.g., HCHB, WellSky, DeVero, Netsmart)
• What is your process for submitting completed coding and reviews?
• Do you provide documentation of rationale for coding decisions and/or OASIS and POC updates?
One of the main benefits of using an outsourced service provider to do your Coding and OASIS review is to take the pressure off of your field staff, and have someone else “connect the dots” for them within the documentation. However, it should also serve as a learning tool for your clinicians. You want the clinicians to understand the recommended changes, play an active part in the review process, and learn from the feedback.
• Do you provide training or feedback to clinicians to improve documentation?
• Do any recommendations or changes you make to the documentation come with an explanation, rationale or reference to the documentation supporting the change?
• Can you assist with ongoing clinician education for OASIS accuracy?
• Do you offer resources or alerts for regulatory changes?
You want to ask your outsource services provider questions around how they are keeping your PHI and other data safe and secure. You should also ask your partner about training and HIPAA compliance, secure workspaces, and ensuring that logins are kept safe and secure.
• How do you ensure HIPAA compliance?
• How often are your staff trained on HIPAA compliance?
• How do you secure your staff’s workspaces, equipment (such as laptops) and logins?
• Do you have a way to communicate with us that is secure (such as encrypted email, or messaging with the EHR platform)?
• What data protection measures are in place for patient information?
• Are you willing to sign a Business Associate Agreement (BAA)?
Want to have a conversation about outsourced services? Contact us today!
CMS Releases OASIS E-2 Guidance Manual
OASIS E-2 is going into effect as of April 1, 2026.
Here is a summary of the key changes from OASIS E-1 to OASIS E-2:
Major Item Changes
1. Transportation item revised
· OASIS E-1: Collected A1250 – Transportation, which asked about lack of reliable transportation and how that affected medical appointments/needs.
· OASIS E-2: A1250 is removed and replaced by a new A1255 – Transportation item to better align with similar items in other CMS post-acute care tools.
2. Gender/Sex item updated
· OASIS E-1: Uses M0069 – Gender.
· OASIS E-2: Replaced by A0810 – Sex (reflects standardized terminology used across CMS instruments).
3. COVID-19 item removed
· OASIS E-1: Included O0350 – Patient’s COVID-19 vaccination is up to date (added in E-1 to support the COVID-19 vaccination quality measure).
· OASIS E-2: O0350 is being removed (the measure or data collection requirement is no longer part of the OASIS data set in E-2).
Additional Timepoint & Item Scope Adjustments
1. New or expanded items at Resumption of Care (ROC)
OASIS E-2 adds A1110 – Language, B0200 – Hearing, and B1000 – Vision to the list of items collected at the ROC time point (previously these may not have been required at ROC).
Skip Patterns and Minor Edits
Some skip patterns and edit logic are modified (e.g., how responses flow between items) due to these item changes.
https://www.cms.gov/files/document/oasis-e2-draft-508-11-14-25.pdf
Suspended Telehealth Face-to-Face Encounters for Home Health and Hospice Providers
Face-to-face encounter requirements are a critical compliance issue for home health and hospice agencies. The government shutdown that occurred as of midnight on January 30th means that the telehealth option for face-to-face encounters has expired. While the current bill in legislation would extend the allowed telehealth face to face, there is no guarantee that it will be made retroactive when the government re-opens. Therefore, home health and hospice agencies should not accept telehealth face-to-face encounters starting January 31st.
Stay tuned here for more updates!
2/4/2026 Update:
The goverment has re-opened and the telehealth waiver has been extended. The extension is retroactive to cover telehealth visits that occurred during the temporary lapse.
Face to Face Requirements
One of the biggest areas of concern we have in our audits, is the Face to Face. There is lack of information, difficulty getting the proper documentation from your referral sources, and risk involved in taking a patient without a valid face to face. Here is a quick checklist for your staff to help them make sure its right!
Home Health Face-to-Face (F2F) Requirements Checklist
1. Timing of Encounter
☐ F2F occurred within 90 days before or 30 days after SOC
☐ Encounter date is clearly documented
2. Qualified Provider Performed Encounter
☐ Encounter completed by one of the following:
☐ Certifying physician
☐ Facility physician (if direct discharge)
☐ Nurse Practitioner (NP)
☐ Physician Assistant (PA)
☐ Clinical Nurse Specialist (CNS)
☐ Certified Nurse Midwife (CNM)
☐ Provider is authorized under Medicare and state law
☐ Provider relationship to certifying physician is appropriate (if NPP)
3. Documentation Requirements
☐ F2F documentation is present in medical record
Documentation includes:
☐ Date of encounter
☐ Provider name/credentials
☐ Clinical findings
☐ Diagnosis/condition addressed
☐ Documentation supports medical necessity
☐ Documentation is legible and complete
4. Relationship to Home Health Need
Documentation clearly explains:
☐ Why patient needs skilled services
☐ How condition limits function
☐ Why homebound status applies
☐ How findings relate to ordered care
☐ Narrative is patient-specific (not generic)
5. Certification Integration
F2F information is incorporated into:
☐ Physician certification
☐ Plan of Care (485)
☐ Verbal/written orders
☐ Certifying physician signed and dated certification
6. Telehealth (If Used)
☐ Telehealth encounter meets Medicare rules (must note it was a video visit, date, time and confirm it was HIPAA-compliant).
☐ Platform is compliant
☐ Encounter is allowable under current policy (check for date of current extension).
☐ Telehealth visit is documented as F2F
How Incorrect Coding Can Cost You
Missed or incorrect codes and OASIS items can reduce home health reimbursement by 10–30% per 30-day period, and it usually comes from how the episode is grouped.
Below is a practical breakdown of where that 10–30% loss actually comes from, with concrete examples.
1. Wrong Primary Diagnosis can mean Wrong Clinical Grouping (10–20% impact)
Under PDGM, the primary diagnosis determines the clinical grouping, which is a major payment driver.
2. Missed Comorbidities = Lost Comorbidity Adjustment (5–20%)
PDGM allows low or high comorbidity adjustments, but only if secondary diagnoses are:
Clinically relevant
Properly sequenced
Reflected in OASIS
3. Incorrect Functional Scoring Alignment (5–15%)
Functional impairment level is calculated from OASIS responses, but:
Diagnosis selection and clinical documentation (especially therapy evals) should support those scores. The OASIS should reflect significant mobility deficits.
Diagnosis list lacks diagnosis to support Functional Impairment.
4. Improper Sequencing (5–10%)
CMS sequencing rules are strict in home health. Common errors include:
Aftercare code sequenced before active condition
Chronic condition sequenced ahead of acute/post-op reason for care
Etiology/manifestation sequencing errors
Sequencing outside of the top 6: Same diagnoses, different order = different payment (due to risk adjustment).
5. Admission Source & Timing Misclassification (5–15%)
Coding affects whether a case is grouped as:
Institutional vs Community and Early vs Late
The highest reimbursement, with all other factors being the same, is Early Institutional.
6. Conservative or “Safe” Coding (10–30%)
Agencies often under code to “avoid audits”. This does not prevent audits—but it can result in underpayment. Some issues include:
Using unspecified codes
Omitting relevant conditions – get these physician-verified and use them!
Avoiding complication codes that are applicable to the patient.
_______________________________________________
Why These Losses Often Go Unnoticed
No denial or rejection
Claims still pay, just at a lower rate
Payment variance not reviewed at episode level
How High-Performing Agencies Prevent This
Use highly qualified, certified Coding and OASIS Reviewers
Encourage your staff to verify any diagnosis that would have an impact
Comorbidity capture checklists
Diagnosis sequencing audits
PDGM case-mix validation reports
Staff education tied to coding and OASIS impact.
License Requirement for MA Home Care Passes House
I had a great conversation yesterday with a staff member of the Home Care Alliance of Massachusetts regarding the bill for licensure for Home Care agencies in the state. This article is a great read with details of what we know so far. "With our aging population expected to grow exponentially in the coming years and the number of family caregivers shrinking, the demand for home care will subsequently increase. It is critical for the Commonwealth to have the proper standards and protections in place for home care agencies to ensure consumers receive quality care and our dedicated home care workers are properly trained and supported in the field. "
I will be watching this closely, as it goes to the Senate. I am looking forward to helping Home Care agencies in MA navigate the new requirements should the bill pass.
https://lnkd.in/eVHitecN